
Why I'm Still Long GRAIL: The Bad Week That Proved the Thesis
I have been a champion of multi-cancer early detection (MCED), and therefore GRAIL, since the beginning. So let me start with a bad week.
In May 2022, when ~400 people received a letter telling them a cancer signal may have been detected. It wasn't true. The letters went out between May 10 and May 18, and more than half of them reached people who hadn't even had their blood drawn yet. For a company whose entire promise is "we will tell you about cancer before it can hurt you," it's hard to imagine a worse headline. The coverage wrote itself: the cancer test that cries wolf.
Here's the thing almost everyone got wrong, and the reason this episode actually deepened my conviction rather than shaking it. It wasn't the test. The erroneous letters were triggered by a software configuration error at GRAIL's telehealth vendor, PWNHealth, a workflow defect in the (key) layer that sits around the assay, not the assay itself. The Galleri laboratory result was never implicated. The failure was in orchestration.
If you have read anything else I have written, you know why I find that almost poetically on-point. Biomarkers don't become markets until they become robust clinical workflows. The future of diagnostics is systems, not tests. Precision medicine is becoming an operations business. GRAIL's worst early week was a demonstration of this thesis. The science worked — and don't get me wrong, the science needs to improve. But more importantly, the operating system around the science failed. That is the entire game, and hopefully, a start-up learning that lesson early and cheaply is a feature, not a bug.
Why MCED is the poster child
Step back from the bad week, because the reason I care about GRAIL has nothing to do with one vendor and everything to do with what MCED is. And that's core to our mission and vision at DeciBio: MCED may be the cleanest example I can point to of what I mean when I say the precision medicine revolution will be driven more by tools and diagnostics than by pharma. The logic is brutally simple: catch cancer early and you are very often fine; catch it late and you are in serious trouble almost regardless of how good the available therapy is.
I put this on a slide for our team in January 2022, as part of a "vivid vision" presentation for where the field was going. I still love this slide!
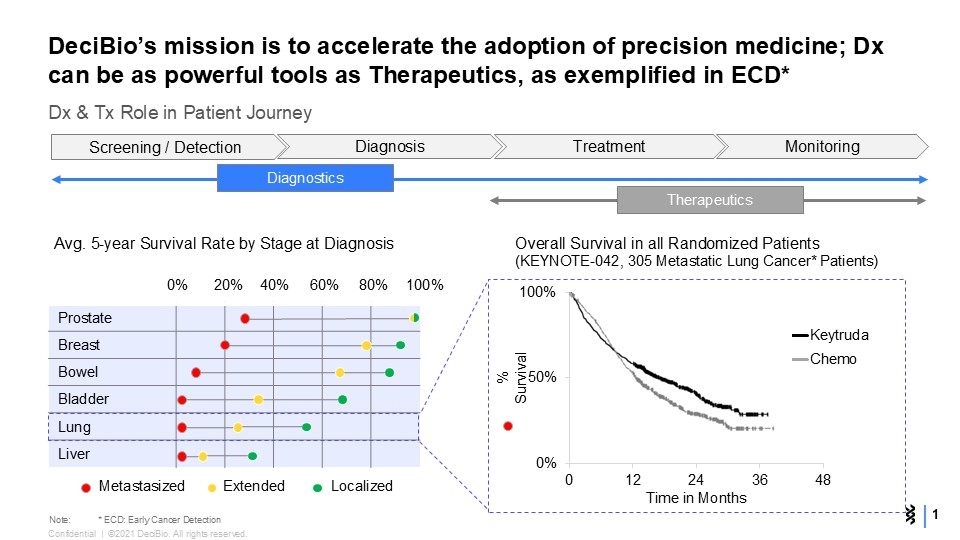
Look at the two panels together. On the left, average five-year survival across six common cancers, sorted by stage at diagnosis. The localized (green) dots sit far to the right, near 80–100% survival. The metastasized (red) dots collapse toward zero. The single biggest determinant of whether you live is not which drug you eventually get. It's what stage you were in when someone found it. On the right, the counterpoint: overall survival from KEYNOTE-042, one of the landmark immunotherapy trials, in metastatic lung cancer. Keytruda versus chemo. This is a genuinely important, practice-changing therapy — Jim Allison received the Nobel Prize for findings tied to that concept — and look how modestly the curves separate, and how low they both land. To be fair, treatment in the real world involves combo-therapies. But still. This is what therapies and pharma can do once the cancer is already advanced. It helps. It is not the same kind of lever as finding the disease while it is still curable.
That sharp contrast is the investment thesis. The red dots are the problem. A test that moves people from red to green — that shifts the stage at which cancer is found — is doing something no metastatic-setting drug can match, because it is operating at the point in the patient journey where the survival curve is still steep. Dx can be as powerful a tool as Tx. In early cancer detection, it can be more powerful.
What I think actually happens from here
Conviction in the category is not the same as naïveté about the product, so let me be specific about what I believe and where I think the real risk sits. None of it is in the science. All of it is in performance, cost, and the operating model.
Single-cancer detection will have its moment, but it's the bridge, not the destination. In the near term, targeted single-cancer screening tests — better colorectal, better lung, better liquid biopsies aimed at one disease — will post real wins, because the evidence bar and the reimbursement story are simpler for one cancer at a time. But it is not the vision. The vision is the one we articulated in the slide: a single blood draw, part of your routine physical, that screens for most cancers at once. The whole reason MCED matters is that ~70% of cancer deaths come from cancers with no recommended screening at all. You don't close that gap one assay at a time. You close it with one draw that looks for everything.
Galleri 1.0 probably isn't the version that wins, far from it — and that's fine. I'll say the quiet part plainly: the first-generation product likely does not have the performance you need to deploy it viably at population scale. The sensitivity-at-acceptable-specificity, and therefore the real-world positive predictive value, just won't justify the cost when you run it across millions of average-risk people. That's not heresy; it's the normal shape of a platform's first act. The honest read is that v1 proves the concept and builds the evidence base, and a later generation — call it v3 — is where the performance and cost curves finally cross into "deploy this to everyone over 50."
And I think getting there requires multiomics. A methylation-only or SNV-only signal is, I suspect, not enough to hit the performance you need at the price you need. The version that moves the needle likely integrates multiple molecular layers — methylation plus fragmentomics plus protein and other signals — because that's what it takes to push sensitivity up at the early stages (where the signal is faintest and the clinical value is highest) without wrecking specificity. The first company to land that multiomic combination, at a cost that survives a payer's spreadsheet, owns the category. A Freenome executive mentioned this to me a couple of years ago: proteomics may be best to detect immune signatures at early cancer stages, and as the tumor size and burden increases, more ctDNA can be detected, typically at later stages.
Why GRAIL is fine — and why the category is better than fine
So when I look at GRAIL's hard years — the false-alarm letters, the Illumina acquisition and regulator saga, and more drama — I see a company that has been through the operational and political wringer while the underlying science kept compounding. The science will improve.
The reason I'm still long the idea, and the company that has the biggest head start at it, is the same reason that bad week in 2022 didn't move me: the failures have all been in the operating system, and operating systems get built. The biology of "early is curable, late is not" is not up for debate. We can discuss lead time bias, which does play a role. But sit with the slide for a moment — the red dots and the flat Keytruda curve — and the whole argument resolves quickly. Maybe GRAIL sorts it out, or maybe someone else will. But we have to win this one if we want to move the needle and win the war on cancer.
This is a personal essay. The views expressed are my own and do not necessarily represent the views of DeciBio, its clients, or any affiliated organizations. Nothing here should be interpreted as investment, medical, legal, transaction, or clinical advice. I have been a longstanding champion of multi-cancer early detection; treat my enthusiasm as a disclosed bias, not a recommendation. The vision slide is from DeciBio, January 2022.